Today was a great day.
I grew up in the prairies, surrounded by farmers and ranchers. When older "Marlboro" men come in the department I get a twinge of familiarity that I get with no other population. It almost makes me a little nostalgic.
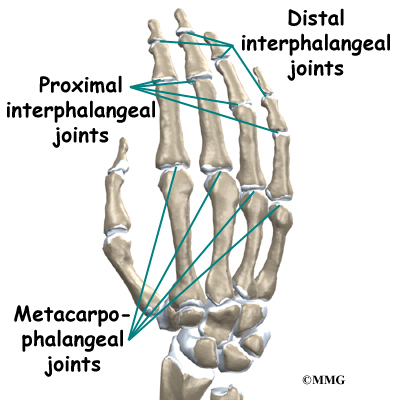
This older, eastern European farmer came in this morning after a tussle with a table saw. His right middle finger was lacerated in several places, including one long lac heading midline from the tip to the DIP joint. The nail was divided into one larger piece and several small flakes, the end of the finger was crushed to a pulp. His second finger had a 2 cm laceration to the lateral aspect, also from tip to DIP. I will admit that when I triaged him I looked at the finger wishing I'd get to be the one that got to repair it, but knew that it was way beyond my skill and experience in the land of sutures. Most of the docs I work with know of my expanded scope from working in the Arctic and thus let me do the straightforward sutures that come into the department.
Warning...if you are queasy about nails (Nature Nerd) you might want to stop reading now because I am going to go into the gory details on this one.
After he'd done the nerve block the middle finger the doc called me into the room and asked if I'd like to freeze the 2nd finger for suturing. I had never worked with this particular doc before but earlier had heard him asking one of the nurses why cardiac bloods had been ordered so I figured he was of the old school 'don't do it unless I order it first' mentality.
So I was pleasantly surprised when he asked me to inject the lido. He said he'd heard that I suture and asked if I'd also like to work through repairing the middle finger.
Inside voice: HELL YEAH! HOLY HOT TAMALE!! SWEET!
Outside voice: Yes, that would be great, if you don't mind walking me through it step by step.
The patient had already had his x-rays so we knew that the saw hadn't cut through the bone. He did the first adsorbable suture and then offered me the needle driver. Eeek! Hadn't done those before. I pieced together what I could inside the boggy tip.
After that we had to remove all of the bits of nail that were still attached. This meant essentially clamping the needle driver onto the end and pulling the nail off the bed. At first I couldn't get the technique but then saw how with rocking it back and forth eventually the nail just comes loose from the nail root and slips out. Feel free to shudder now.
*Shudder*
Then the nasty part which was separating the nail from the nail bed which was still attached. If you want to see a video showing how this is done...voila. Yeah. He did a couple passes under the nail with the scissors...that is correct...scraping the nail from the nail bed, then offered me the scissors.
Just...couldn't...do...it.
I was completely embarrassed but I was just concentrating on my breathing at that point.
I was getting that flushing feeling that comes over me just before I pass out...needed to breathe...did someone turn up the heat? Make the room smaller? Shine the light on my head?
I am blaming it on my low blood sugar but really it was just too much at that exact moment. I had just ripped off the other half of his nail for crying out loud! This was already a big day for me! I was starting to feel like a torturer in a Burmese prison.
Anyway, the sensation quickly passed (thank goodness--but not until after the patient joked that he hoped I wasn't planning on becoming a surgeon...har har). I was back at it to put in the sutures to close up the nail bed, the tip of the finger, and the rest of the laceration that went from the cuticle down to the first knuckle. Because the nail was so badly damaged and the patient didn't care if he ever regrew a nail, we did not reattach what remained.
So it was a nice close up to the nail bed, but it looked pretty hectic after that. To me, it was a thing of beauty! My first complicated laceration repair. I wanted to take a photo of it, but since I had no "before" to dazzle people with, I thought the "after" might leave some people wondering what I was so damn proud of.
I sutured the other finger, which was much more straight forward, though my first time ever going through the nail with a stitch. (Also super cool!)
Ahhh...it was so rewarding, and I learned so much during the procedure. Plus the doc was keen to teach and was very patient going through everything with me. The patient was really great about the procedure as well. He had actually apologised for coming into the department, telling us that it would have probably healed fine on it's own. He was sorry for bothering us.
We hastily reassured him that injuries like his are what ED are made for, and he could come in anytime without guilt with a chief complaint like that.
Sigh...salty old tough-as-nails farmers...gotta love 'em.
{kind=link}
8 comments:
Still shuddering!!!!
I used to be a theatre nurse (OR nurse) before I became a paramedic. By the time I left nursing I was proud to say that I had worked in every different speciality of theatres and could scrub for anything that came through the door.
Gunshot to the face - no problem!
Traumatic amputation of a leg - no problem
Radical Vulvectomy - no problem!
You get the picture right??
Zadeks procedure (removing the big toe nail) - you've got to be kidding me!!!! NO WAY!
I would do my very best not to even be in the theatre at that point.
How the hell did you do that????
Got to go now, feeling a little nauseous.
It's funny what will set one off. The other day, I was doing an ABG on a patient by myself for the first time. I'd done several with supervision, and was now alone with the patient, digging around in his wrist with a needle. I started to feel like I was going to faint. I was alternately amused and pissed off, but decided that the better part of valour was removing the needle and going for help, rather than passing out on the floor with the needle still in his arm.
That really is awful.
Damn, new blog posting and I don't even get to read it. Thanks for the heads up though!
Medic--Hahahaha! Yeah, it's funny how certain things just go beyond our desensitization threshold. Really, I was having a tough time with it in the beginning but I think it was partly because I was chatting with the guy and built somewhat of a rapport with him. It wasn't just walking into the room and dealing with a finger poking out of a sterile drape.
BB--Yeah, sometimes it is better to face the embarrassment of bailing on something over the embarrassment of fainting on top of a patient!
Especially if you passed out AFTER hitting the artery! ;)
I had to take a moment in the bathroom during my first autopsy, and was so PISSED at myself because it was so interesting and it wasn't bothering me on a conscious/cognitive level AT ALL!
I was mortified when the med student came in to check on me. Sigh. Good times.
Ry--Sorry! :)
NN--Hahaha--yes I remembered you running around the Cozy Cabin covering your ears and yelling "lalalalalalal" when I told you about my toe nail issues in Morocco. Figured you'd have a meltdown if you read the gory details of this post. :)
I'm so proud of you.
That's awesome!
I hope I don't pass out when my first business case to create a health promotion dietician position gets approval from NHS London! LOL - our profesh careers are so different and wonderful. That said, you would have been proud of me today, when I arrived to provide homecare to a homeless gentleman at a shelter, and noticed another gentleman in the foyer with two black, sloughing, gangrenous necrotic toes walking barefoot towards the mess hall. Nothing like an impromptu stabilization dressing and trip to the ER... only to find that he's competent and refusing to have surgery. Now we will be seeing two gentlemen in the homeless shelter, one for diabetes management and another for IV antibiotics and autolytic debridement, and daily dressings, until either he dies or we can convince him to return for appropriate treatment. Fun Fun Fun.
Love you mean it!
Lalalalala. Is this post over yet?
Hand lacs are fun! Nail removal is not...
While your suturing remember not to lock your knees and to keep breathing. The tendency is to hold your breath and lock your knees because you're totally focused on making sure your sutures are pretty for the attending...it happens all the time to med students on Surgery and OB/GYN.
Post a Comment